
One of the most common questions I get from patients concerns their cholesterol levels. They want to know whether their cholesterol is high, and if so, what that means for them.
Of course, their cholesterol level in and of itself isn’t really what worries them. What they actually want to know is, Am I going to have a heart attack? What about a stroke?
Those are the right questions. But a cholesterol number alone doesn’t always give us enough information to answer them well.
Yes, there is a real correlation between cholesterol and cardiovascular risk, but that doesn’t mean all cholesterol will harm you. LDL cholesterol (often known as “bad” cholesterol) carries the most risk, while HDL cholesterol has protective qualities. Triglycerides play a role, too.
That said, even a high LDL reading doesn’t automatically indicate heart disease. And cholesterol-lowering medications come with real downsides in cost, inconvenience, and side effects.
So how do we figure out when to prescribe medication? Let me share my approach.
Know the Connection: Cholesterol, Plaque, and Heart Disease
First, we need to understand how cholesterol contributes to cardiovascular disease to begin with.
When LDL cholesterol accumulates in the artery walls, it forms what we call plaque. Initially, plaque is soft and vulnerable to breaking off. If a soft plaque does break free and travels downstream to the heart’s smaller vessels, it can lead to a heart attack.
To protect against this, the body deposits calcium into soft plaque to harden it and make it less likely to break off. This hardened plaque is less likely to cause problems by breaking away and blocking vessels. It accumulates over time, however, narrowing the diameter of arteries and restricting blood flow (a process called atherosclerosis). Eventually, this can lead to blockages as well.
Cholesterol blood tests tell us how much cholesterol is circulating in the blood at a given time. What they can’t tell us is whether this atherosclerotic process is already underway.
Imaging for Cholesterol Clarity
Instead of treating patients solely on the basis of an LDL number, I may recommend imaging to get a better picture of their cardiovascular health. Then I can see if urgent and aggressive intervention is needed or if attempts at lifestyle modification could be sufficient.
The Coronary Artery Calcium Score: A Non-Invasive Closer Look
The coronary artery calcium score is a specialized CT scan that indirectly identifies the amount of blockage in your arteries based on the calcium your body has put down in the soft plaque. If you receive a score of zero, that indicates you have no calcium in your arteries and, likely, no plaque buildup.
The test does carry about a 10 or 15% possibility of a false negative, since a coronary calcium score can only detect calcified plaque, not soft plaque. But for the great majority of people, a score of zero means that, at this point, you have no buildup of plaque.
The CT Angiogram: When More Information Is Needed
Since the coronary calcium score is unable to detect soft plaque, an additional test may be beneficial for patients with greater risk factors for cardiovascular disease, such as a family history of heart disease or a personal history of diabetes. For these patients, a CT angiogram can illuminate early soft plaque accumulation.
The process for a CT angiogram is similar to that of the calcium score. The main difference is the use of contrast dye injected into the bloodstream so the heart’s vessels light up on the scan, allowing us to physically see the amount of blockage that exists.
This test also comes with a risk of false positives and false negatives. Sometimes, for example, it may underestimate certain arteries. In general, however, it provides a good idea of both the soft and hard plaque in your arteries.
The trade-off of a CT angiogram is a higher risk of side effects due to the use of IV contrast. It also typically has a higher cost. The benefit is that we get early insight into cardiovascular disease before it reaches a problematic stage and can treat accordingly.
The most definitive test for detecting arterial blockage is still considered cardiac catheterization, in which a physician uses a thin, flexible tube to physically enter the arteries and evaluate them. This test carries more risk, but it is the gold standard for finding out how the arteries are faring.
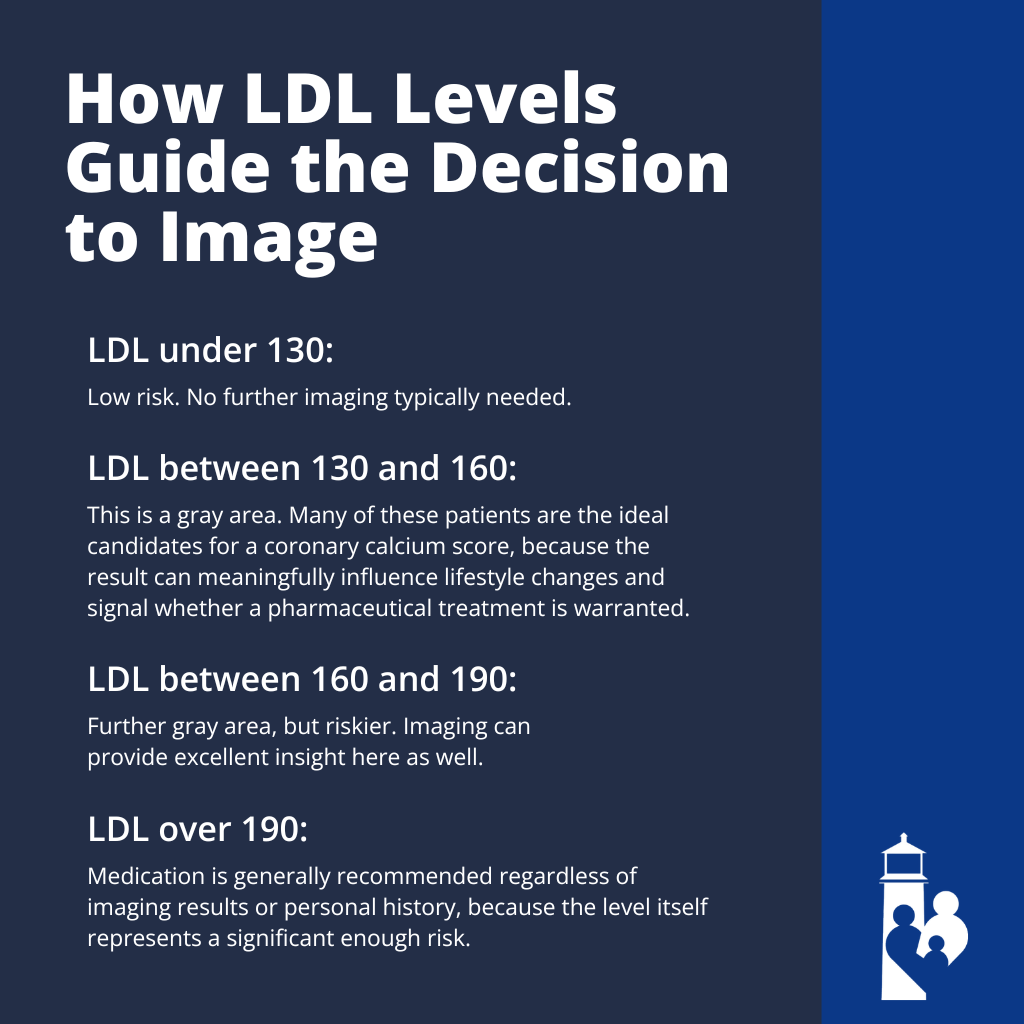
How LDL Levels Guide the Decision to Image
Not every patient with an elevated LDL needs further imaging. Below is a general framework I use for determining when to image for patients without existing heart disease or major risk factors:
- LDL under 130: Low risk. No further imaging typically needed.
- LDL between 130 and 160: This is a gray area. Many of these patients are the ideal candidates for a coronary calcium score, because the result can meaningfully influence lifestyle changes and signal whether a pharmaceutical treatment is warranted.
- LDL between 160 and 190: Further gray area, but riskier. Imaging can provide excellent insight here as well.
- LDL over 190: Medication is generally recommended regardless of imaging results or personal history, because the level itself represents a significant enough risk.
Further numbers to know:
- For those with known coronary artery disease, we generally want to see an LDL below 55, and medication is almost always part of the equation.
- For those with no existing disease but with a personal history of major risk factors like diabetes, we aim for LDL below 100 and focus on lifestyle modification first.
Treat the Person, Not the Number
From my earliest medical training, I was always taught to treat people, not numbers. A cholesterol test is a number; it needs to be put into a context.
Consider a patient with an LDL of 165, a family history of relatives living into their late 90s, no high blood pressure, no diabetes, and a calcium score of zero. Putting that person on a medication with real potential side effects makes little sense. Lifestyle modification is the right answer.
On the other hand, patients with risk factors or elevated LDL sometimes struggle to change their habits. Seeing concrete evidence of early plaque buildup in their own arteries may be the motivation they need to alter their lifestyle more aggressively.
About 80% of medical problems can be improved through lifestyle changes, but such changes are often the hardest to accomplish. Imaging can make the stakes feel real in a way that a number on a lab report can’t.
Why I Don’t Order Every Test Available
Though I appreciate tests like the calcium score and CT angiogram and find them useful, I don’t order every test for every person.
Why?
First, I always ask myself: What will I do with the result? If it won’t change how I treat the patient, I typically don’t order it.
Second, every test has costs, and not just monetary. Beyond the financial side, an abnormal result can trigger more tests, which can lead toward increasingly invasive procedures, each carrying its own risks. It’s a pattern worth being cautious about.
Cardiac imaging can be a powerful tool in the right context. But recommendations should always depend on the individual: their LDL levels, their personal and family history, their risk factors, and what we plan to do with the result.
Final Thoughts on Cholesterol, Medication, and Heart Disease
Deciding whether someone needs cholesterol medication isn’t as simple as reading a number off a lab report. An elevated LDL needs to be put in the context of who that person is, what their history looks like, and what the imaging shows.
Cardiac imaging, particularly the coronary artery calcium score, gives us a meaningful data point for patients in the gray area of treatment recommendations. For the right patient, it can be the difference between starting an unnecessary medication and confidently pursuing lifestyle change instead.
If you have questions about your cholesterol or whether imaging might be right for you, I encourage you to bring it up during your appointment. The right answer always depends on you as an individual.
